|
|
|
|
| DOES
HYDROCHLORIC ACID RENDER IONIC-COLLOIDAL SILVER INEFFECTIVE? |
|
To
view second page sub titles please click on them, to open in separate
window. |
|
Following a lead by the US FDA in banning all products containing colloidal silver (3) associated with health information, the South African Department of Health falsely misrepresents the facts and claims that "all over-the-counter products containing colloidal silver or silver salts are not recognised as safe and effective" and that "indiscriminate use of colloidal silver has resulted in cases of argyria, a permanent discoloration of the skin and deep tissues" as well as "neurological deficit, and renal and metal fume? damage". (4) It is noteworthy that prestigious journals such as the Lancet, the British Medical Journal and the Journal of the American Medical Association have for decades attested to the safety and efficacy of traditionally far more crude "grind method" colloidal silver, commonly several thousand % more concentrated (5) yet equally less effective than the micro electro-colloidal silver used today. (1) The lie behind this suppressive move against the public’s access to this simple health protective substance is revealed by the fact that there is not a single case of argyria in modern medical history as a result of electro-colloidal silver. All reference to this and other toxicities, on careful checking, leads directly to the "abuse" of orthodoxy sanctioned old medical silver products, usually not even colloidal silver (and if so, by the grind method), and mostly in the form of medicinal nose drops, capsules, pills, gum, pulverisers etc, or in cases of severe toxicity, intravenous injections in gram-plus quantities in animal experiments. (6) The lie is perpetuated by the FDA and the likes of Messrs Fung, Bowen and Barrett, and the world’s only contemporary argyria victim, Rosemary Jacobs, who was poisoned more than forty years ago by "silver nose drops of unknown composition". (5) Fortunately, the Gaia protocol colloidal silver..., incorporating the immuno-essential elements, Cu, Zn & Mn, dynamically synergised with hydrogen peroxide, is still legally accessible locally (7) via an inexpensive strategic water purification and fortification treatment unit, resulting from a far-sighted leading edge local development paralleling advanced international water research and treatment trends. Both silver and also hydrogen peroxide (especially in combination) exhibit significant microbial inactivation at concentrations that do not pose any health risk according to the EEC, WHO and US EPA. (8) The EEC, WHO and Israel Ministry of Health have specifically approved the use of colloidal silver as a drinking water disinfectant at an MCL (Maximum Contaminant Level) of 80 ppb. (8) Switzerland, Germany and Australia have given approval for the use of a commercial formulation of colloidal silver and hydrogen peroxide as a drinking water disinfectant. (8) The US EPA has declared that silver does not cause adverse health effects and has set a Maximum Level at 100 ppb for all drinking water. (9) A new European Union Drinking Water Standard in draft form has removed any upper limit for silver in drinking water following the WHO’s Guidelines for Drinking Water Quality which states that "it is not necessary to recommend any health-based guidelines for silver as it is not hazardous to human health". (9) One teaspoon (5ml) of 1 ppm colloidal silver in a glass (250ml) of water equals 20 ppb. Since the guidelines relate to lifetime exposure for even the most susceptible sub-groups, calculated at 2 litres a day, one could safely consume 8 glasses each with 5 teaspoons (25 ml) of 1 ppm of colloidal silver every day. The most commonly used quantity is a mere teaspoon in a glass of water 3 or 4 times daily. Clearly the FDA / MCC itself is more hazardous to health!
References & Internet Hyperlinks
WE ADVANCE THE COUNTER
Dear Frank, Ivan and List members Frank wrote in response to Ivan: > Ivan, > Well lets see, exactly how does HCl ionize Ag without forming AgCl? > What am I missing? > frank key >An experiment testing the (zero) solubility of silver in hydrochloric acid >pH=2, same strength as found in the stomach, is available. >frank key
ST: Are you not, to your peril, ignoring the potential role of aqueous ammonia in this equation, whereby I strongly suspect it plays a transmutational role in the chemistry of the biological passage of silver into the body (and I expect, its utility there, under the continued influence of ammonia as well)? I note that Frank's latest experiment is once again conducted in vitro, with no attempt to approach the complexity that exists in the real world, not even the temperature is adjusted. The test medium is free of any organic material, including bacteria and hence is sterile. Under these unnatural conditions it would have been possible to attempt to measure the medium for silver, but instead, a less sensitive measure of weight is used. Is it not conceivable that the contaminants in the HCL and or from dissolved gasses over the 26 hour period could have replaced liberated silver atoms with other elements, making a silver assay more definitive? More importantly,
from my perspective, would be the possible role of ammonia, if
not in a limited experiment of this nature, then certainly in
the case of determining the possible bio-availability of AgCl,
which Frank maintains is insoluble and hence is not utilised in
vivo.
Date: Wed, 21 Feb 2001 Dear Frank and List members. Frank is conveniently ignoring the role of aqueous ammonia when simplistically claiming that silver chloride (AgCl) formed on contact of ionic colloidal silver with stomachic hydrochloric acid is insoluble and hence inactive in the body, indeed not assimilated at all. Frank has recently reiterated this claim, stating: "Once silver chloride is formed, which is instantly upon contact, then it is a compound, not dissociated silver ions and chloride ions in solution. So the silver chloride acts as a compound which is insoluble in the blood". I argue(d) that ammonia plays a transmutational role in the chemistry of the biological passage of silver into the body and its utility there. Ammonia is a good solvent for AgCl (The Merck Index; Hawley's Condensed Chemical Dictionary; Columbia Electronic Encyclopedia)(Ongoing series undated). By tying up silver ions and forcing extensive dissociation of molecular silver chloride, ammonia pulls silver chloride into aqueous solution (Encyclopedia Britannica). Solid AgCl can be dissolved and separated from complexation by aqueous ammonia and is quite soluble in concentrated solutions, until it dissolves to the point at which the Ag ion is present even as a separate species in solution (Zumdahl S, Chemical Principles). AgCl is only a slightly soluble salt, but ammonium salts are highly soluble (Plambeck J, Introductory University Chemistry I, University of Alberta). Frank rejected this ammonia hypothesis with the snide remark that: <"A human body containing enough ammonia to dissolve silver is way past needing colloidal silver">. I might legitimately state the converse, but such a response is non-productive. Whilst Frank claims that silver 'ions' are ineffective in vitro, he also claims that "his" silver 'particles' are effective. There has been much debate around the definition of an ion, and my contribution is that "an ion is an atomic or molecular 'PARTICLE' having a net electrical charge" (Mc Naught A, Intnl Union of Pure and Applied Chemistry Compendium of Chemical Terminology, Blackwell Science, 1997). Perhaps Frank should rename his "particle" to clarify exactly what it is. Frank calculates the fate of silver, be it ions or particles, only in the stomach and blood and then only theoretically from a test tube extrapolation, yet the former is the mere first step in its journey into bio-complexity. It appears that Frank is intent on oversimplifying the biochemistry of silver so as to maintain consistency with a preconceived commercial strategy of one-upmanship over more conventional forms of electro-colloidal silver. I find this rather disappointing for a professing professional scientist. Frank's in vitro AgCl argument is so simplistic that they have not progressed even to the level of a basic chemistry set experiment, which at least might have demonstrated the ammonia phenomenon. I restate my in vivo ammonia hypothesis in a little more detail, since Frank has not scientifically or logically countered it. Some time ago, I wrote: "In many ways the alimentary canal is to us what the soil is to the plant. Minerals (as 'particles' or ions) form chelates or complexes with organic chemicals, such as organic acids, amino acids, proteins and others. Complexing agents may also help to dissolve sparingly soluble inorganic substances by complexing one or more of the products of dissociation, thus shifting the chemical equilibrium in favour of solution. Since naturally occurring complexing agents are of biological origin, their formation by microbes can help bring minerals into solution, and consequently into absorption." Sadly, Frank refuses to consider ecology, physiology or biochemistry in his stubbornly blinkered approach to this AgCl bioavailability puzzle. In a functional human body, ammonia plays an important role in health. Ammonia is commonly found in rainwater, in rivers at usually less than 6 ppm. Soil typically contains about 1 to 5 ppm of ammonia and after fertiliser application, more than 3000 ppm (obviously elevating water levels from run-off). Food and water is absorbed into the bloodstream and is carried throughout your body within minutes. You can taste ammonia in water at levels of about 35 ppm. Lower levels than this occur naturally in food and water. The FDA determined in 1973 that the levels of ammonia and compounds normally found in food do not pose a health risk; ammonia is necessary for normal functions. Maximum allowable levels in processed foods are: 3.2% ammonium bicarbonate; 2.0% ammonium carbonate; 0.6-0.8% ammonium hydroxide; 1.1% dibasic ammonium phosphate. (Agency for Toxic Substances and Disease Registry, Public Health Statement, December 1990) Ammonia is my chief candidate as a viable means to rendering silver bound as AgCl soluble once again in the colon and also systemically once absorbed. I shall identify some perceived weaknesses in Frank's argument. Frank presents an over-simplified test-tube case and considers only total silver chloride vs total ammonia in his rejection of my ammonia hypothesis. This is also reflected in his recent very selective presentation of "Normal Laboratory Values", in which the 'plasma' value for ammonia (point 17- point 80 ppm) and the 'serum' value for chloride are given. As previously stated, even common fasting values are up to10mg/100ml in saliva, 4mg/100ml in gastric juice and 0.3mg/100ml (3 ppm) in whole blood (Documenta Geigy Scientific Tables), far higher, more realistic and meaningful figures than Frank's, but this is by no means my main point. Firstly, these values would have little bearing on treating illness, since the values are for a healthy population and so would apply only to prophylactic silver usage, and even then only with very limited extrapolatory value, since silver assimilated into the body, even though quickly rendered relatively insoluble within the high internal chloride mille, would become more available as the acidosis which precedes and accompanies most illnesses and certainly most infectious conditions, increases, rendering silver chloride soluble relative to the degree of acidosis and consequential ammonia buffering response. The purine nucleotide cycle moreover, although present in many types of tissue, is normally particularly active in muscle and during vigorous exercise, blood concentrations of ammonia can increase five-fold (Salway J, Metabolism at a Glance; Ament W, et al, Int J Sports Med, Jan, 18(1), 1997) Frank underplays the normal concentrations of and ignores the potential peak concentrations of ammonia in the human body, especially during infectious illness and in particular the importance of ammonia concentrations at certain sites in the body, such as at the colonic lumen and the liver and kidneys. Frank also ignores the significant chloride secretory inhibition effect of ammonium at the epithelium of the colonic mucosa where silver must be at its smallest molecular potential in order to be assimilated. Perhaps a better comparison than the transitional product ammonia with chloride, which widely interacts with other elements and is critical in many normal bodily processes, would be nitrogen, the ammonia substrate, which is twenty times more abundant than chloride in the human body (Documenta Geigy, Scientific Tables). Chronic metabolic acidosis enhances ammonium re-adsorption due to increased NH4+ production. The mechanism of ammonia secretion by diffusion furthermore confers ability to this buffer system to replenish itself. Prolonged acidemia causes increased uptake of glutamine into tubular epithelial cells and subsequent metabolism into NH4+ and HCO3-. This flexibility of the ammonia-ammonium buffer system to increase excretion of NH4+ ten-fold from 30 mEq/day to well over 300mEq/day, is the predominant means of acid excretion in chronic acidosis. (Guyton A, Textbook of Medical Physiology; Rose B, Clinical Physiology of Acid-Base and Electrolyte Disorders) Normal serum ammonium concentrations are in the range of 20-40 mM but can increase in illness until at about 400 mM it causes alkalosis and neurotoxicity (King M, Medical Biochemistry, Terre Haute Center for Medical Education, 1998). Ammonia is readily, indeed reliably formed in vivo via oxidative deamination and also by transmination in the alimentary canal, primarily in the colon, by breakdown of proteins (including blood from intestinal bleeding) to amino acids and deamination by normal bacterial enzymes (Harrison's Principles of Internal Medicine) and is actively absorbed, converted and recycled via the ornithine (urea) cycle (Goodman & Gilman's: The Pharmacological Basis of Therapeutics). Thus excretion of ammonia counteracts blood acidosis and conserves alkaline reserve. When living things die, including food products, host cells and micro-organisms, their nitrogenous remains are “mineralized”, ie converted into inorganic forms of nitrogen, mainly ammonia (Lewis O, Institute of Biology Studies in Biology, Series 166, 1986), which is formed in quantity by putrefactive micro-organisms in the secum and colon and is "absorbed" into the body (Prosser C, Comparative Animal Physiology). The colon, unlike most organs, is "normally" exposed to high concentrations of ammonia, a weak base that exerts profound and diverse biological effects on mammalian cells. The colonic lumen normally contains up to 70 mM, actively inhibiting chloride secretion in the colon, the transport event which hydrates mucosal surfaces. (Prasad M, et al, J Clin Invest, 96(5), 1995; Hrnjes B, et al, Gastroenterol 110, Suppl, 1996; Mayol J, et al, Am J Physiol 273 (Cell Physiol 42), 1997; Miyata R, et al, Inflamm Res, 48(5), 1999) Cell membranes are generally highly permeable to small, lipophilic molecules such as ammonia (Walter F, et al, J Experiment Biol, 196(1), 1994). Ammonia is an endogenous inhibitor of intestinal chloride secretion and is equally effective mucosally and serosally (O'Brien T, et al, Digest Disease Week, 3355, 1998). Colon cells are subjected to high concentrations of NH3 and NH4+. A sizeable portion of this buffer is absorbed (Raminez M, et al, Pflugers Arch (Eur J Physiol), 438(4), 1999). Ammonia profoundly inhibits Cl secretion in human intestinal epithelia, with half-maximal inhibition at 4-6 mM. The lumen of the lower gastrointestinal tract is the setting for bacterial action on ingested protein and the colon consequently experiences concentrations of the protein degradation product ammonia that may reach 100 mM. (Hrnjez B, et al, Amer J Physiol, 277(3), 1999) Frank has also recently stated that: <"Silver chloride forms very large molecules and larger yet particles which are removed by the kidneys">. Now, a pertinent question for Frank: IF ONLY SILVER IONS ARE COMPOUNDED WITH CHLORIDE TO FORM INSOLUBLE AgCl, HOW THE HELL DOES THE SILVER CHLORIDE, WHICH YOU STATE IS NOT ASSIMILATED INTO THE BODY, FORM LARGE PARTICLES AND GET INTO THE KIDNEYS, LET ALONE HOW IS IT REMOVED FROM THE KIDNEYS IF IT IS SO INSOLUBLE? I have reasonably shown that both feats are possible only because of previously postulated complexations and the action of ammonia. Since silver is NOT present in the urine in measurable quantities, even after intravenous injection (Casarett and Doull's Toxicology), it must be rendered soluble by ammonia and reabsorbed into the body. Regards Stuart
Date: Mon, 5 Mar 2001 08:24:32 Dear Roger, Frank and List members Some time ago, we discussed Frank's silver chloride hypothesis and later my counter ammonia hypothesis. Roger threw a further wobble Frank's way when he reported measuring high urinary silver levels following an intensive course of ionic colloidal silver. Frank assumed that the major silver excretion was unabsorbed silver chloride in the feces, but Roger actually observed, first high urinary levels, followed by high fecal excretion, putting a lid on that one of Frank's flights of fantasy. Roger, I need to question the 6ppm, however, since although it is antagonistic to Frank's silver chloride hypothesis and complementary to my ammonia hypothesis, it does not correlate well with the published records. Roger wrote to Frank: "The concentration of silver in my urine reached 6 PPM in the first sample taken 5 days after stopping CS intake". ST: I don't doubt that the silver was in the urine, but the 6ppm seems much higher than the "trace" generally found in the literature, even in industrial and medical settings. Bear in mind that besides certain circumstances possibly influencing acidosis and ammonia buffering, it should also be borne in mind that ammonia production increases progressively in the bladder and in the sample flask over time and that this could lead to increased solubility of trace Ag, in turn increasing detectable Ag as per my ammonia hypothesis, thereby explaining the relatively high urinary readings, even though silver is not actively excreted in urine. Frank wrote to Roger: "This could also mean that ions made it to the bloodstream where they combined with chloride and the kidneys filtered out the silver chloride which is passed with urine (as has been speculated by some, who shall remain nameless)". ST: Earlier I asked Frank: "IF ONLY SILVER IONS ARE COMPOUNDED WITH CHLORIDE TO FORM INSOLUBLE AgCl, HOW THE HELL DOES THE SILVER CHLORIDE, WHICH YOU STATE IS NOT ASSIMILATED INTO THE BODY, FORM LARGE PARTICLES AND GET INTO THE KIDNEYS, LET ALONE HOW IS IT REMOVED FROM THE KIDNEYS IF IT IS SO INSOLUBLE"? I have received no reply to date. I note that Frank wished to believe that: "If most of the silver was found in the feces, that would be consistent with high ionic silver forming silver chloride in the GI tract and not being absorbed". One problem for Frank: The fecal silver came later than the urinary, meaning that relatively high concentrations of silver completed a systemic circuit. This is clearly contrary to your (Frank's) silver chloride hypothesis. Again I beg an answer to the previous question. I have reasonably shown that both feats (urinary and secondary fecal presence) are possible only because of previously postulated complexation and the action of ammonia. Since silver is "not" present in the urine in 'relatively' significant quantities, it must be rendered soluble by ammonia and reabsorbed into the body. If the silver chloride hypothesis does not hold, I believe it legitimately submits to the ammonia hypothesis. Roger, the source which I referred to previously as saying that: "Silver is NOT present in the urine in "measurable" quantities, even after intravenous injection", was from Casarett and Doull's Toxicology: The Basic Science of Poisons, Fourth Edn, 1991, McGraw-Hill (Health Professions Division), edited by Amdur, Doull and Klaasen. This a classic text, regularly updated and what it specifically says (direct quote) is that: "The major route of (of silver - species unidentified) excretion is via the gastrointestinal tract. Urinary excretion has NOT been "reported" to occur even after intravenous injection". My more accurately formulated position therefore is that silver in urine has been detected in traces only, ie barely measurable and always relative to total assimilated and excreted silver. This is confirmed in another classic and oft cited paper (DiVincenzo G, et al, Int Arch Occup Environ Health, 56(3), 1985) (detailed further on) which in the biological monitoring of workers exposed to different species of silver, concluded that silver is eliminated predominantly in the feces, since urinary concentrations did not differ measurably from controls. I submit the following additional details in support of this contention: Absorbed silver appears mostly associated to blood cells and globulins and is cleared by the liver. Silver that is not cleared may deposit in the liver, but also in other organs. Fecal elimination was found to have two phases: During the first phase the half-life was 1 day, which probably corresponds with the initial fast clearance of unabsorbed silver in the feces. In the second phase the half-life was 48-52 days, and has been fairly conclusively identified with the liver clearance. (Jongerius O and Jongeneelen F, Criteria document for metallic silver. CEC. Occupational exposure limits; EUR 14314; 1992) Silver is absorbed from the intestine and partially excreted in the kidney.
Random Urine: 0-0.46 nmol/L; 24 Hour: 0-0.61 nmol/d, Method of Analysis: High Resolution ICP/MS, London Health Sciences Centre.
Results Reporting: Ranges for females from birth and up in ug/L: Normals: Low 0 High 3.4 Ranges for males from birth and up in ug/L: Normals: Low 0 High 3.4 In a biologic monitoring study of workers exposed to different species of silver, atomic absorption spectroscopy analysis revealed a mean silver concentration in the <blood> of 1.10 ug/L, in <urine> at less than 0.005 ug/G, and in feces at 15 ug/G. Comparatively, the concentrations in controls were less than 0.5 ug/L in the >blood>, less than 0.005 ug/G in the <urine> and 1.5 ug/G in the <feces>. (DiVincenzo G, et al, Int Arch Occup Environ Health, 56(3), 1985) In a cross sectional study of precious metal powder workers, 92% had raised <blood> silver concentrations in the range of 0.5-62 ug/L with a mean 10 ug/L, whilst 96% had raised <urinary> silver concentrations in the range of 0.5-52.0 ug/L with a mean of 11.3 ug/L (Rosenman K, et al, Br I Ind Med, 44(4), 1987). In atomic absorption spectrophotometric monitoring of silver levels in silver sulfadiazine cream treated burn patients, the concentrations of silver in subjects without industrial or medical exposure was less than 2.3 ug/L in the <blood> and 2 ug/Day in <urine>. In silver sulfadiazine (SSD.cream treated patients, <plasma> concentrations reached a maximum of 310 ug/L and in <urine>, a maximum of 400 ug/Day. (Wan A, et al, J Clin Chem, 37(10 Pt 1), 1991) Tentative reference values for the biologic fluid content of therapeutic metals, proposed on the basis of the most representative studies, suggest that the variability in normal subjects range up to 10 ug/L in whole <blood> and up to 1 ug/L in <urine> (a 10:1 ratio) (Perrelli G and Piolatto G, Sci Total Environ, 120(12), 1992). As can be seen from the above studies and standard values, silver concentrations can vary quite considerably. However, the highest urinary value in these studies still falls far short of your 6ppm = 6 milligram/L <urinary> figure. The Rosenman study showed a maximum <urinary> value of 52ug/L = 0.052 milligram/L, which is still a hundred times (1000%) less than your reading. I would advise that you check my comparisons since conversions are definitely not my strong point. If my figures are correct and you cannot produce data to the contrary, then I suggest that you or someone else with the means to do so, conduct appropriate tests to determine accurate comparative concentrations in the blood, urine and feces for ionic, mixed and pure particulate silver, since this remains the only means of definitively proving or disproving Frank's silver chloride hypothesis, already fairly well demolished by the considerable, but patchy evidence already at hand. It is in the interest of all who work with colloidal silver to help settle this matter for once and for all. Regards Stuart
Date: Wed, 14 Mar 2001 Dear Roger and List members Since yours is apparently the only data available for CS, and 6ppm figure is so high, I simply felt compelled to check the figure and circumstances, especially since your observations led you to conclude that: "Silver is excreted easily from the body, primarily in the urine". I doubt very much whether this is true generally for silver (species undefined), or even specifically for colloidal or ionic silver. However, it is of course possible that silver is secreted primarily in the urine under certain circumstances. You are not happy with my using other exposures as comparatives, but in the absence of more appropriate data, this is the only means we have of gathering a perspective on your data, which comparative method is scientifically valid, if not ideal. I did however consider the Rosenman study to represent the highest urinary reading in the subsets previously provided, stating that it "showed a maximum urinary value of 52ug/L = 0.052 milligram/L, which is still a hundred times (1000%) less than your reading". I could have calculated from the Wan study which had a 400ug/Day maximum, but I did not feel confident to extrapolate a 400ug/Day figure to 400ug/L, but I suppose, assuming a passing of one litre a day, such an extrapolation is not unreasonable for rough comparisons. Some of the previous data was for burn patients, where the application of silver to large surface areas of weeping, blood vessel rich tissue, leads to relatively high blood and urinary levels compared to other exposures, indicating that ionic silver is appreciably assimilated into the bloodstream and is subsequently excreted. Having searched further, I have found another such study indicating relatively high urinary levels. It is interesting that these burn studies have used urinary analysis. Fecal values are not presented, indicating, as per the following Boosalis study, that there might be circumstances involved which favour urinary excretion, leading researchers to conclude that: "The 24-hour urinary excretion of silver appears to be a very sensitive indicator of cutaneous absorption in these patients". What factors are at play, both in your study and these burn studies, compared to the studies of other exposures? Could it simply be the most obvious common denominator, namely ionic silver? Do you now see the potential value of comparative studies, even if they are of quite different circumstances? Any way you look at it, our man Frank's silver chloride hypothesis is shot to pieces by the sheer weight of the evidence. It is in fact we, not Frank, who are engaging in true science. For the record, the confirmatory topical silver burn study follows: Although silver sulfadiazine has been used extensively as an effective topical antimicrobial agent in thermal injury patients, little is known about the cutaneous absorption of the silver moiety in these patients. Therefore, we longitudinally evaluated both serum silver concentration and 24-hour urinary excretion of silver in 23 patients with second- and third-degree thermal burns. Mean serum silver concentrations were modestly elevated throughout the patients' hospital course. Urinary excretion of silver was markedly elevated, especially in those patients with more severe burns. Indeed, in patients who had burns covering more than 60% of the total body surface area mean peak silver excretion was 1100 micrograms/24 hr (normal, less than 1 micrograms/24 hr). Thus, silver ion is absorbed across the burn wound in thermal injury patients treated with silver sulfadiazine. The 24-hour urinary excretion of silver appears to be a very sensitive indicator of cutaneous absorption in these patients. (Boosalis M, et al, Serum and urinary silver levels in thermal injury patients. Surgery, 101(1), 1987) Please note the maximum figure of 1100ug/Day highest in the most severely burnt patients. This is still five times less than your maximum figure. I guess that I need not point out that, as with our colloidal silver, the silver in question entered the body as silver ions, as did presumably all of the SSD studies provided and these are therefore quite appropriate as comparatives. However, bearing in mind that the SSD ions did not have the stomachic hydrochloric acid to deal with, your figure of 6mg/L still remains incredible, and even though it would serve to support my ammonia hypothesis all the more strongly, I would still suggest that we could improve the science of colloidal silver appreciably by replicating your experiment or even better, conducting tests capable of determining accurate comparative concentrations in the blood, urine and feces for ionic, mixed and pure particulate silver. Furthermore, by delineating the circumstances leading to the detection of such relatively high urinary values, this phenomenon proves beyond a shadow of doubt, that ionic silver is effectively assimilated into and circulated within the body. Regards Stuart
Date: Mon, 19 Mar 2001 12:57:03 Dear List members: Herewith an update on the abovementioned topic. Frank Key's "silver chloride hypothesis" states that hydrochloric acid in the stomach renders insoluble the ionic silver (largely produced by conventional CS generators).
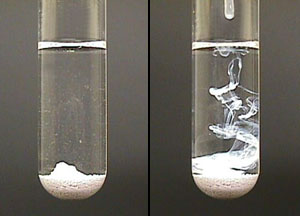
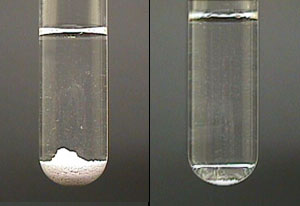
System: AgCl system
Chemical Explanation: The addition of AgNO3 increased the concentration of silver ions in solution. This increased the rate of the forward reaction. As a result the equilibrium shifted to the right. In doing so more AgCl precipitate is formed. Frank implies that this proves that most colloidal silver is useless, or useful only to the degree that such colloids also contain traces of what he calls “particles of silver”, which latter he estimates is usually less than 1% of such colloids and which he states nevertheless is entirely responsible for the anecdotal efficacy of such colloids. He also states that his process produces no ionic silver, but rather 100% particulate silver, with the unstated, yet obvious implication that his process is 99+% more effective. Since this flies in the face of the practical experience of all serious researchers as well as thousands (actually millions) of casual users of conventional CS, I sought an explanation and proposed a counter “ammonia hypothesis”. Frank’s response to my critique of his hypothesis and to my counter proposal has been to insult me rather than defend his position. I have resorted to challenging that I shall assume that his inability to defend means submission to the ammonia hypothesis. Still no defence, just more insults. I recently remarked that: “Frank’s in vitro AgCl argument is so simplistic that it has not progressed to the level of a basic chemistry set experiment, which at least might have demonstrated the ammonia phenomenon”. The URL (and the photo) provided above illustrates Frank’s hypothesis. Clicking on the NH3 symbol on that page will show you my counter argument to Frank’s hypothesis (the photo is reproduced below), which he conveniently neglected to take account of and still stubbornly refuses to acknowledge, resorting to insults instead of scientific defence of his failed hypothesis.
The text for this section reads: System: AgCl system Observations: The addition of NH3 solution caused the white precipitate of AgCl to disappear. Chemical
Explanation: The addition of NH3 decreased the concentration
of free silver ions in solution. This decreased the rate of the
forward reaction. As a result the equilibrium shifted to the left.
In doing so more AgCl precipitate dissolved (photo above). For an additional verification of the above experiment using pure silver chloride and the addition of ammonia in colour from a chemistry textbook, see photo below. The text reads ~ Aqueous ammonia is added to silver chloride (white). The silver chloride, insoluble in water, dissolves to form Ag(NH3)2+(aq) and Cl-(aq) (silver ammonia and chloride) (Reference: Steven Zumdahl Ph.D [Professor
of Chemistry, University of Illinois] Chemical Principles, D.C.
Heath and Co, 1992, pg 315)
For the remainder, my in vivo ammonia hypothesis data (also) remains unchallenged and hence I deem the "silver chloride hypothesis" to submit to the "ammonia hypothesis", both in vitro under certain conditions and invariably in vivo. I add the following as further proof that silver ammonia solutions are feasible in vitro and by extension, in vivo, and also some facts as they relate to the production and concentration of ammonia in the gut as well as systemically, in particular during abnormal conditions of ill-health. Consider for example, the Procedure for Deactivation of Ammoniacal Silver Solutions: Dilute the silver/ammonium solution with 15 parts of water for every one part of solution (15:1 water: silver/ammonium solutions). In another container, make a 5% hydrochloric acid solution. Slowly add the HCl solution to the silver/ammonium solution until the pH reaches 2. Stir frequently. When the pH reaches 2, silver chloride should begin to precipitate out. (Office of Research Safety, Northwestern University) Looking at this procedure to precipitate out silver chloride, it is evident that a pH of approximately 2 is required before the process is begins in earnest. In reality, the reverse of the above scenario actualy takes place in vivo (in the alimentary canal). Silver combines with chloride to become insoluble silver chloride. In the case of saline manufactured colloids, the silver chloride formation simply starts weakly during production, ie before contact with the HCl. However, as has been seen, this process is dependent on the relative presence of sufficient HCl and absence of ammonia. Sufficient HCl produces high acidity, but usually this is short-lived, even in the stomach. Frank Key would have us believe that this is the end of the line for ionic silver. However, the ecology of the alimentary canal quickly changes in favour of the reverse. The pH of HCl in the stomach is between 1-3. When food enters the stomach, pH may rise to 4.0 due to the buffering capacity of proteins (Winsemius, 1998). On duodenal drainage, pH is already 5.5-7.5 (Normal laboratory values - The Merk Manual). After food enters the duodenum, bicarbonate ions are secreted to neutralize and alkalinize the food mixture. The pH of the small intestine is generally in the region of 8.0. (David Winsemius, M.D., BA (physics), MPH) Although kidney and muscle may liberate ammonia, most is of gut origin with << portal vein concentrations greatly exceeding systemic levels >> (Cordoba J & Blei A, Am J Gastroenterol 92, 1997). Muscle wasting may potentiate hyperammonemia. In liver disease, portal blood ammonia is not converted efficiently to urea. Gut-derived ammonia is produced by action of bacterial flora on dietary protein and on epithelial and bacterial debris, as well as mucosal secretions containing urea, amino acids, amines, peptides and purines. Protein overload may lead to increased ammonia. (Summerskill W & Wolpert E, Am J Clin Nutr 23, 1970: Dasani B, Am J Gastroenterol, 93(5), 1998; Wolf D, Encephalopathy, Hepatic from Medicine, Ob/Gyn, Psychiatry, and Surgery/Gastroenterology, Topic update Aug 14, 2000. eMedicine.com, Inc. 2001) Factors which contribute to increasing blood levels of ammonia or produce hyperammonemia are the use of sedatives, antidepressants, and antipsychotic agents, electrolyte imbalances, gastrointestinal bleeding, excess dietary protein, constipation, and hypokalemia-induced renal production, or renal failure (Fessel J& Conn H, Gastroenterol, 62, 1972; Vince A, et al, Clin Sci Molec Med, 51,1976; Conn H, et al, Gastroenterol, 72, 1977; Vince A & Burridge S, J Med Microbiol, 13, 1980; Weber F, et al, J Lab Clin Med, 110, 1987; Wolf D, Aug 2000, eMedicine.com). Diuretics increase the movement of NH3 into cells (Kramer L, et al, Hepatology, 31(1), 2000). Early studies of patients with liver disease reported increased gastric urease activity associated with elevated gastric and blood ammonia levels and the frequent colonization of the upper small bowel with urea-splitting bacteria (Rappoport W & Kern F, J Lab Clin Med, 61, 1963; Fleshler B & Gabuzda G, Gut, 6, 1965; Lal D, et al, Gastroenterol 62, 1972). << Infection and drugs are also sources of ammonia>>, and a late rise in its level after cure of Helicobacter pylori infection could reflect progressive liver disease with less synthetic function (Baertl J, et al, J Clin Invest, 42, 1963). Ammonia levels increase as liver function decreases (Rikkers L, et al, Gastroenterol, 75, 1978). Increased levels of ammonia may enter the systemic circulation because of portosystemic shunting (Wolf D, Aug 2000, eMedicine.com). Although ammonia synthesis is usually attributed to fecal bacteria, the stomach, which possesses strong activity when infected with Helicobacter pylori, is an alternative site from whence urea readily diffuses from blood into the gastric lumen where, in the presence of H. pylori, it is hydrolyzed to ammonia, which is then rapidly absorbed and contributes to higher circulating blood ammonia levels (Neithercut W, et al, J Clin Pathol 46, 1993; Gubbins G, et al, Am J Gastroenterol, 88(11), 1993; Ito S, et al, Eur J Gastroenterol Hepatol 6, 1994; Mokuolu A, et al, Am J Gastroenterol, 92, 1997; Dasani B, Am J Gastroenterol, 93(5), 1998; Realdi G, et al, Digestive Diseases and Sciences, 44(2). 1999). The presence of blood in the upper gastrointestinal tract from gastrointestinal bleeding results in increased ammonia and nitrogen absorption from gut. Blood transfusions too, may result in mild hemolysis with resulting elevated blood ammonia levels (Wolf D, Aug 2000, eMedicine.com). If the aforementioned in vitro phenomenon are not convincing because these studies relate only directly to ammonia, and not directly to silver chloride, consider a recent Russian article dealing with <<< the management of patients with purulent infection with intravenous infusions of silver chloride ammonia solutions >>> (Abrosimov I, et al, Khirurgiia (Mosk), 7, 1997). (No Medline abstract is available, but the title informatively reads: <<< “THE MANAGEMENT OF
PATIENTS WITH PURULENT INFECTIONS WITH INTRAVENOUS INFUSIONS OF So much for Frank Key's nonsense. Regards Stuart Admittedly we have not
reproduced a debate here, the reason being that the individual
proposing the silver chloride hypothesis refused to defend it
beyond those remarks repeated in the text. The original debate
may still exist on the net at the silverlist
|
|||||||||||||||



| |
||
|
||
| |
||
|
Gaia is copyright © 2006 Gaia all rights
reserved Designed by Webs The Way |
||
|
Page Counter as of January 2008 |